What if low testosterone isn’t the root problem — but a warning signal?
Over the last decade, more men than ever have been told they have “low T.” Prescriptions for testosterone replacement therapy (TRT) have risen sharply. Clinics promise restored energy, libido, muscle mass, and vitality.
But here’s the deeper question:
Why is testosterone low in the first place?
What if low testosterone isn’t simply a hormone deficiency — but a reflection of something happening at a deeper metabolic level?
In many cases, low testosterone is not an isolated endocrine problem. It is a marker of metabolic dysfunction.
Understanding this changes everything — from how we interpret lab results to how we approach treatment.
Let’s unpack why.
The Modern Low Testosterone Epidemic
Population studies consistently show declining testosterone levels across generations. Even after adjusting for age, men today have lower testosterone than men the same age decades ago.
At the same time, we’ve seen a dramatic rise in:
- Obesity
- Visceral fat accumulation
- Insulin resistance
- Type 2 diabetes
- Chronic low-grade inflammation
- Poor sleep
- Sedentary lifestyles
These trends are not coincidental.
Low testosterone and metabolic dysfunction often travel together.
But correlation does not equal causation. So what’s the relationship?
How Metabolism and Testosterone Are Connected
To understand the link, we need to briefly look at physiology — in a way that’s accessible but accurate.
1. Insulin Resistance Suppresses Testosterone
When insulin levels are chronically elevated (hyperinsulinemia), several things happen:
- The liver reduces production of sex hormone-binding globulin (SHBG)
- Lower SHBG leads to lower total testosterone levels
- High insulin directly impairs testicular Leydig cell function
For clinicians: hyperinsulinemia also alters hypothalamic-pituitary-gonadal (HPG) axis signaling and may reduce LH pulsatility.
In simple terms:
When insulin is constantly high, testosterone production and regulation suffer.
This is why men with metabolic syndrome frequently present with low total testosterone.
2. Visceral Fat Converts Testosterone to Estrogen
Not all fat is equal.
Visceral adipose tissue — the fat stored around abdominal organs — is metabolically active.
It contains high levels of the enzyme aromatase, which converts testosterone into estradiol.
More visceral fat → more aromatization → lower circulating testosterone.
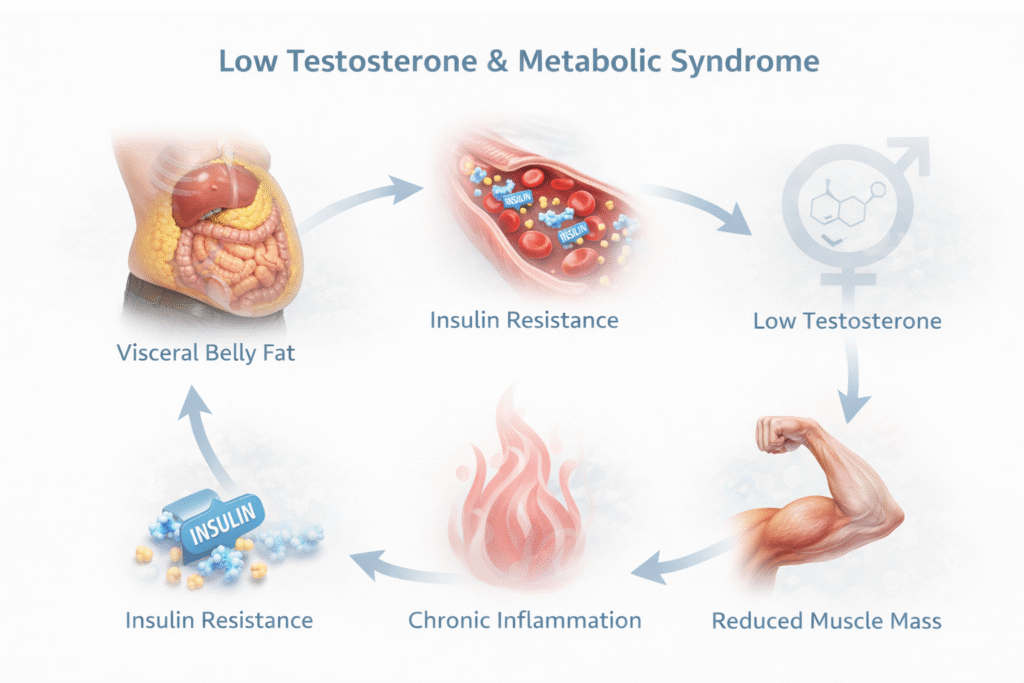
This creates a feedback loop:
- More fat lowers testosterone
- Lower testosterone makes it harder to maintain muscle mass
- Reduced muscle mass worsens insulin resistance
- Insulin resistance promotes more fat storage
A vicious metabolic cycle.
3. Chronic Inflammation Disrupts Hormonal Signaling
Metabolic dysfunction is characterized by chronic low-grade inflammation.
Adipose tissue releases inflammatory cytokines such as:
- TNF-α
- IL-6
These inflammatory mediators interfere with:
- Hypothalamic GnRH signaling
- Pituitary LH release
- Testicular steroidogenesis
For patients:
Inflammation essentially “tells” the body it’s under stress. Reproduction and anabolic hormone production become lower priority.
The body shifts into survival mode.
4. Sleep Disruption and Testosterone
Testosterone secretion follows a circadian rhythm and is closely linked to deep sleep.
Obesity and metabolic dysfunction are strongly associated with:
- Obstructive sleep apnea
- Reduced REM sleep
- Fragmented sleep cycles
Even one week of sleep restriction can significantly reduce testosterone levels.
If metabolism is impaired and sleep quality declines, testosterone declines with it.
Is Low Testosterone the Cause — or the Consequence?
This is where the conversation becomes nuanced.
Low testosterone can worsen metabolic health by:
- Reducing lean muscle mass
- Increasing visceral fat accumulation
- Decreasing insulin sensitivity
So yes, testosterone deficiency can contribute to metabolic dysfunction.
But in many men, the timeline suggests:
Metabolic dysfunction appears first.
Testosterone decline follows.
Rather than asking, “How do we replace testosterone?” we might first ask:
“Why did the system downregulate testosterone?”
The body is rarely random.
Signs and Symptoms Patients Should Recognize
Low testosterone symptoms often overlap with metabolic symptoms, including:
- Persistent fatigue
- Reduced libido
- Erectile dysfunction
- Loss of morning erections
- Decreased muscle mass
- Increased abdominal fat
- Low motivation
- Brain fog
But here’s the important part:
If these symptoms occur alongside:
- Weight gain (especially abdominal)
- Elevated fasting glucose
- High triglycerides
- Low HDL
- High blood pressure
It’s very likely the issue is systemic metabolic dysfunction — not isolated hormone failure.
When Is Testosterone Replacement Appropriate?
There are cases where TRT is clearly indicated:
- Primary hypogonadism
- Testicular failure
- Genetic conditions
- Persistently low testosterone with significant symptoms despite optimized metabolic health
But prescribing testosterone in the presence of untreated metabolic dysfunction can be like:
Putting premium fuel into a damaged engine.
It may temporarily improve symptoms — but it does not repair the underlying metabolic disturbance.
That doesn’t mean TRT is wrong.
It means TRT without addressing insulin resistance, visceral fat, inflammation, and sleep is incomplete.
The Practical Strategy: Fix the Metabolic Terrain
If low testosterone is often a marker of metabolic dysfunction, the logical approach is:
Improve the metabolic terrain.
Here’s what that looks like.
1. Reduce Visceral Fat
The most powerful intervention for increasing testosterone naturally is reducing central adiposity.
Even a 5–10% weight loss can significantly increase testosterone levels.
Focus on:
- Caloric awareness
- Prioritizing protein intake
- Reducing ultra-processed foods
- Managing alcohol intake
2. Improve Insulin Sensitivity
Strategies include:
- Resistance training (2–4x per week)
- Increasing daily movement (NEAT)
- Structured carbohydrate intake
- Time-restricted eating (if appropriate)
- Optimizing fiber intake
Resistance training is particularly potent.
It improves insulin sensitivity and directly stimulates testosterone production.
3. Prioritize Sleep
Aim for:
- 7–8 hours nightly
- Consistent sleep-wake cycles
- Screening for sleep apnea if risk factors are present
In some men, treating sleep apnea alone significantly improves testosterone levels.
4. Lower Chronic Inflammation
- Whole-food diet
- Omega-3 fatty acids
- Adequate micronutrients (zinc, magnesium, vitamin D)
- Stress management
- Reducing visceral fat
Inflammation reduction restores healthier endocrine signaling.
A Reframing: Testosterone as a Barometer
Think of testosterone like a barometer.
It reflects:
- Energy availability
- Metabolic efficiency
- Inflammatory load
- Sleep quality
- Body composition
When these systems are healthy, testosterone tends to normalize.
When these systems are stressed, testosterone declines.
Instead of viewing low testosterone as a failure of masculinity or aging alone, we might see it as:
A message from the body.
The Big Takeaway
Low testosterone is often not an isolated hormonal disease.
It is frequently a biological signal of metabolic dysfunction.
Before reflexively replacing testosterone, we should ask:
- Is insulin elevated?
- Is visceral fat excessive?
- Is inflammation high?
- Is sleep disrupted?
Because in many men:
Improving metabolic health improves testosterone naturally.
And even when TRT is used, outcomes are better when the metabolic foundation is strong.
Final Thought
Testosterone does not usually fall without reason.
The body does not downregulate anabolic hormones randomly.
Low testosterone is often the smoke — not the fire.
If we only treat the smoke, we miss the opportunity to extinguish the fire.
And that is the difference between symptom management and true metabolic restoration.
People Also Ask
Is low testosterone a sign of metabolic dysfunction?
Yes, in many men low testosterone is not an isolated hormone problem but a sign of underlying metabolic dysfunction. Conditions such as insulin resistance, visceral fat accumulation, chronic inflammation, and poor sleep can suppress testosterone production. In these cases, low testosterone often reflects impaired metabolic health rather than primary testicular failure.
Can insulin resistance lower testosterone levels?
Yes. Chronically elevated insulin levels can reduce sex hormone-binding globulin (SHBG) and impair normal hormonal signaling in the hypothalamic–pituitary–gonadal axis. Over time, insulin resistance is strongly associated with lower total and free testosterone levels.
Will losing weight increase testosterone naturally?
In many overweight or obese men, weight loss—especially reduction of visceral abdominal fat—can significantly increase testosterone levels. Studies show that improving insulin sensitivity, increasing muscle mass, and reducing inflammation can partially or fully restore testosterone without hormone replacement therapy.
Should I start testosterone replacement therapy if my levels are low?
Not always. If low testosterone is caused by metabolic dysfunction, addressing underlying factors such as obesity, sleep apnea, poor diet, and inactivity may improve levels naturally. Testosterone replacement therapy may be appropriate in confirmed hypogonadism, but treatment decisions should consider overall metabolic health.
What tests should be done if testosterone is low?
A proper evaluation should include morning total testosterone, free testosterone, SHBG, LH, and estradiol. Because low testosterone is often linked to metabolic issues, testing fasting insulin, glucose, lipid profile, and markers of inflammation can help identify the root cause.
Author bio
Morteza Ariana is a Functional Nutrition Practitioner specializing in insulin resistance, type 2 diabetes, and systems-based metabolic restoration. His work focuses on identifying upstream drivers of metabolic dysfunction — including insulin load, liver–gut axis disruption, circadian misalignment, and micronutrient gaps — rather than masking symptoms.
He works with high-performing professionals through a structured 12-week Metabolic Restoration Blueprint designed to restore metabolic flexibility and long-term resilience.
If this resonates, the next step is clarity.
The Metabolic Restoration Blueprint is a structured 12-week framework designed to correct upstream metabolic drivers — not just manage symptoms.
Scientific References
Low Testosterone and Metabolic Syndrome / Insulin Resistance
1. Corona et al., 2011
Low testosterone syndrome protects subjects with high cardiovascular risk burden from major adverse cardiovascular events
Journal of Sexual Medicine PubMed
2. Laaksonen et al., 2004
Testosterone and sex hormone–binding globulin predict the metabolic syndrome and diabetes in middle-aged men
Diabetes Care
Prospective Finnish cohort study showing low testosterone predicts development of metabolic syndrome and type 2 diabetes. PubMed
3. Stellato et al., 2000
Testosterone, sex hormone–binding globulin, and the development of type 2 diabetes in middle-aged men
Diabetes Care PubMed
Another foundational longitudinal study linking low testosterone to future diabetes.
Mechanisms: Insulin, SHBG, and HPG Axis Suppression
4. Pitteloud et al., 2005
Relationship between testosterone levels, insulin sensitivity, and mitochondrial function in men
Diabetes Care PubMed
5. Selva et al., 2007
Insulin decreases SHBG production by activating hepatic lipogenesis
Journal of Clinical Investigation
Obesity, Visceral Fat & Aromatase
6. Vermeulen et al., 1999
Estradiol in elderly men
Journal of Clinical Endocrinology & Metabolism
7. Grossmann, 2011
Low testosterone in men with type 2 diabetes: significance and treatment
Journal of Clinical Endocrinology & Metabolism
Inflammation and Testosterone Suppression
8. Maggio et al., 2006
Interleukin-6 and testosterone in older men
Journal of Clinical Endocrinology & Metabolism
Shows inverse relationship between IL-6 and testosterone.
9. Kelly & Jones, 2013
Testosterone and obesity
Obesity Reviews
Bidirectional Relationship: Cause or Consequence?
10. Traish et al., 2011
Testosterone deficiency and metabolic syndrome: A vicious cycle
International Journal of Clinical Practice
Weight Loss & Testosterone Improvement
11. Corona et al., 2013
Weight loss improves testosterone levels in obese men: a meta-analysis
European Journal of Endocrinology
12. Khoo et al., 2013
Comparing effects of low-energy diet and exercise on sexual and erectile function in obese men
Clinical Endocrinology
Sleep and Testosterone
13. Leproult & Van Cauter, 2011
Effect of 1 week of sleep restriction on testosterone levels in young healthy men
JAMA