Normal blood sugar but insulin resistance already developing — this combination is far more common than most people realize, and far more dangerous than most doctors communicate. Your body can maintain perfectly normal fasting glucose for years, even decades, while insulin quietly rises higher and higher to compensate. By the time your blood sugar finally tips into the abnormal range, insulin resistance has typically been present for 10 to 15 years.
Many people have normal fasting blood sugar while already developing insulin resistance. This happens because the body can keep glucose normal for years by producing increasing amounts of insulin — masking early metabolic dysfunction until the system can no longer compensate.
They hear this sentence at the doctor’s office:
“Your blood sugar is normal. Everything looks fine.”
And yet, years later, they are suddenly diagnosed with type 2 diabetes.
From the patient’s perspective, the disease seems to appear out of nowhere.
From a physiological perspective, this is almost never true.
What actually happened is that the body compensated silently for years — until it could no longer keep up.
The problem is not that doctors are careless.
The problem is that we are often measuring the wrong signal.
Why Blood Sugar Can Be Normal Despite Insulin Resistance
Blood glucose is tightly regulated because the brain depends on it.
The body will go to great lengths to keep glucose within a narrow range.
It can do this for a long time by simply producing more insulin.
Two people can have the same fasting glucose value:
- Person A needs very little insulin to maintain it → metabolically healthy
- Person B needs three to five times more insulin → already metabolically dysfunctional
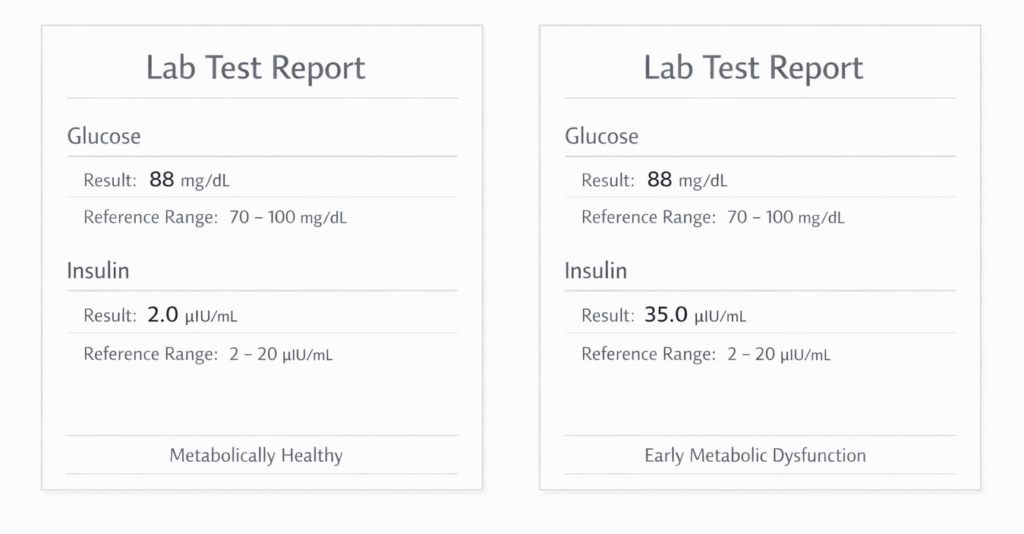
The glucose number looks identical.
The physiology underneath is completely different.
But in most healthcare systems, including here in Germany, we only measure glucose.
We do not ask:
How much insulin was required to keep it normal?
That question is where early disease becomes visible.
The Long Compensation Phase of Insulin Resistance
Type 2 diabetes does not develop suddenly.
It develops gradually, often over 10–15 years.
During this phase, the body compensates by increasing insulin output to maintain normal glucose levels. This often leads to a predictable pattern:
- Fasting insulin rises (but is rarely measured)
- Post-meal insulin responses become exaggerated
- Fat begins accumulating in the liver (NAFLD)
- Triglycerides slowly rise
- HDL cholesterol often declines
- Visceral fat increases
- Energy levels decline
- Blood pressure creeps upward
- Hunger becomes more difficult to regulate
The system is under strain, but still functioning.
Because glucose remains “normal,” patients are reassured:
“Everything looks fine.”
Then one day, the pancreas can no longer sustain the required insulin output.
Glucose finally rises.
And the diagnosis appears to arrive “out of nowhere.”
To the patient, it feels sudden.
Biologically, it was years in the making.
For a full physiological framework of insulin resistance, see our comprehensive insulin resistance physiology framework
Why Normal Blood Sugar Leads to Missed Insulin Resistance
This is why so many people say:
“But my blood sugar was always normal.”
They are not imagining things.
They are describing a real limitation of our current screening model.
Conventional testing is good at detecting established disease.
It is much weaker at detecting early dysfunction.
The result:
- Patients feel gaslit
- Trust erodes
- People blame themselves
- Opportunities for prevention are missed
Not because people failed — but because the system looked too late.
Labs That Reveal Insulin Resistance Despite Normal Blood Sugar
If the goal is early detection, different markers become more informative than fasting glucose alone.
Some examples:
- Fasting insulin
Reveals how hard the pancreas must work to maintain glucose - HOMA-IR
A simple calculation using fasting glucose and insulin that estimates insulin resistance - Triglycerides and HDL together
Often reflect underlying metabolic flexibility and liver function - Evidence of fatty liver (NAFLD)
A strong early signal of metabolic dysfunction, often present years before diabetes - Waist circumference and visceral fat
Better predictors than weight alone
These markers do not replace clinical judgment.
They support earlier insight into what is happening beneath the surface.
See also Why the TG:HDL ratio Exposes Hidden Insulin Resistance
This is not about blaming doctors
It’s important to say this clearly:
Most physicians are working within guidelines, time constraints, and systems they did not design. They are not malicious. They are not careless.
The issue is structural.
Modern medicine is optimized for:
- Diagnosing established disease
- Managing acute problems
- Treating clear pathology
It is less optimized for:
- Detecting early dysfunction
- Understanding slow physiological drift
- Interpreting patterns across systems
This is not a moral failure.
It is a design limitation.
Why Early Insulin Resistance Matters for Prevention
If we only intervene once glucose is elevated, we are intervening late.
If we begin paying attention to:
- Rising insulin
- Early liver changes
- Lipid patterns
- Fat distribution
- Sleep disruption
- Energy instability
We gain the possibility of true prevention, not just disease management.
Most people do not suddenly become diabetic.
They become metabolically strained long before the diagnosis appears.
Metabolic Health Beyond Blood Sugar Numbers
Metabolic health is not simply:
“Is your blood sugar within range?”
It is more accurately:
How resilient is your system at managing energy over time?
That resilience is reflected in:
- How much insulin is needed
- How flexible fuel usage is
- How well sleep supports regulation
- How well the liver handles energy flow
- How stable hunger and energy feel
- How much visceral fat accumulates
These are biological patterns, not moral judgments.
Closing perspective
Many people are told everything is fine — until suddenly it isn’t.
Not because they failed.
Not because they were irresponsible.
But because early dysfunction often remains invisible when we look only at late markers.
If we want real prevention, we need to look earlier.
We need to look deeper.
And we need to understand that “normal” numbers do not always mean healthy physiology.
Frequently Asked Questions
Can you have insulin resistance with normal blood sugar?
Yes. This is very common. In early insulin resistance, the body compensates by producing more insulin to keep glucose normal. Blood sugar may stay in range for years while metabolic dysfunction progresses silently.
Why don’t doctors routinely measure fasting insulin levels?
In many healthcare systems, fasting insulin is not part of standard screening guidelines. Medicine is often structured around detecting established disease rather than early dysfunction, which limits early identification.
What is hyperinsulinemia?
Hyperinsulinemia refers to chronically elevated insulin levels. It is often one of the earliest physiological changes in metabolic dysfunction and can exist long before blood glucose becomes abnormal.
What is HOMA-IR?
HOMA-IR (Homeostatic Model Assessment of Insulin Resistance) is a calculation using fasting glucose and fasting insulin to estimate insulin resistance. It can provide useful insight into early metabolic changes.
Can fatty liver occur without obesity?
Yes. Non-alcoholic fatty liver disease (NAFLD) can occur in people who are not visibly overweight, especially when metabolic dysfunction is present.
Is HbA1c enough to assess metabolic health?
HbA1c reflects average blood glucose over time, but it does not reveal how much insulin the body must produce to maintain that level. It is therefore a late marker, not an early one.
Author bio
Morteza Ariana is a Functional Nutrition Practitioner specializing in insulin resistance, type 2 diabetes, and systems-based metabolic restoration. His work focuses on identifying upstream drivers of metabolic dysfunction — including insulin load, liver–gut axis disruption, circadian misalignment, and micronutrient gaps — rather than masking symptoms.
He works with high-performing professionals through a structured 12-week Metabolic Restoration Blueprint designed to restore metabolic flexibility and long-term resilience.
If this resonates, the next step is clarity.
The Metabolic Restoration Blueprint is a structured 12-week framework designed to correct upstream metabolic drivers — not just manage symptoms.
Scientific References
I’m not citing random blogs. I’m grounding this in serious literature
Foundational insulin resistance & hyperinsulinemia
- Reaven GM. Role of insulin resistance in human disease. Diabetes. 1988.
- Kraft JR. Diabetes Epidemic & You. Trafford Publishing.
- DeFronzo RA. Insulin resistance, lipotoxicity, type 2 diabetes and atherosclerosis. Endocrine Reviews. 2010.
Hyperinsulinemia as early pathology
- Corkey BE. Banting Lecture 2011: Hyperinsulinemia: cause or consequence? Diabetes. 2012.
- Erion KA, Corkey BE. Hyperinsulinemia: a cause of obesity? Current Obesity Reports. 2017.
NAFLD and early metabolic dysfunction
- Samuel VT, Shulman GI. Nonalcoholic fatty liver disease as a nexus of metabolic disease. Cell Metabolism. 2018.
- Yki-Järvinen H. Non-alcoholic fatty liver disease as a cause and a consequence of metabolic syndrome. The Lancet Diabetes & Endocrinology. 2014.
Fasting insulin, early risk & compensation phase
- Ferrannini E, et al. Insulin resistance and hypersecretion in obesity. Journal of Clinical Investigation. 1997.
- Weyer C, et al. The natural history of insulin secretory dysfunction and insulin resistance in the pathogenesis of type 2 diabetes. Journal of Clinical Investigation. 1999.
Triglycerides, HDL, and metabolic risk
- McLaughlin T, et al. Use of metabolic markers to identify insulin-resistant individuals. Diabetes Care. 2003.
- Gaziano JM, et al. Triglycerides, HDL, and risk of myocardial infarction. Circulation. 1997.