Your TG HDL ratio — triglycerides divided by HDL cholesterol — is one of the most informative numbers hiding in plain sight on your standard blood panel. Most doctors never mention it. Yet a ratio above 2.0 is one of the strongest early indicators of hepatic insulin resistance available without any additional testing, and it can be elevated for years before your fasting glucose or HbA1c show anything concerning.
Most of the people who eventually find their way to me don’t come in saying,
“I’m sick.”
They come in saying something closer to:
“I’m functioning… but not the way I used to.”
They’re professionals, usually disciplined, responsible, and health-conscious. They’ve already improved their diet at least once. Many of them exercise. Some even track sleep or wear a CGM for a while.
They’ve also been to their doctor — sometimes several times.
The conversation usually goes like this:
- Labs are “mostly fine”
- LDL is “high”
- triglycerides are “slightly elevated”
- HDL is “okay, but could be better”
They’re told:
“You’re not in a danger zone. Try to lose a little weight, eat less fat, and we’ll re-check in a few months.”
And for a while, they try harder.
But life continues to change underneath:
- energy fades in the afternoons
- concentration feels duller
- the waist thickens, even if the scale barely moves
- carbs feel heavier post-meal
- motivation and resilience decline
They don’t feel broken — just off-track, like their physiology no longer matches the person they remember being.
By the time they sit across from me, they’re not asking for a diet.
They’re asking for a coherent explanation.
And when we zoom out — symptoms, lifestyle, lab trajectory, waist pattern — the same constellation appears again and again.
That is where the TG:HDL ratio stops being just a number on a page and starts becoming a window into a metabolic story no one else has taken the time to read.
When ‘Normal’ Labs Don’t Match Your Body’s Reality
“Your labs can appear normal on paper — yet your body signals fatigue, belly fat, and metabolic stress that no one bothered to explain.”
Most conventional interpretations emphasize LDL and total cholesterol. But for thousands of adults, especially high-achievers with creeping metabolic symptoms, the deeper story often lies in a metric that rarely gets attention: TG:HDL ratio.
Evidence shows the TG:HDL ratio is associated with insulin resistance and atherogenic lipid patterns, even before conventional markers like LDL become severely abnormal. (ScienceDirect)
This article explains
- what TG:HDL actually signifies in metabolic biology
- why it’s clinically relevant
- how it connects mechanistically with hepatic insulin resistance and carbohydrate-induced hypertriglyceridemia.
What the TG:HDL Ratio Really Means (In Simple Terms)
Before we talk about ratios and risk, we need to understand the pieces.
What is a triglyceride?
A triglyceride is basically a package of energy your body moves around in the blood.
- When you eat too much refined carbohydrates than your liver converts some of that excess carbs into triglycerides.
- Those triglycerides are loaded into particles (VLDL) and released into the bloodstream.
In scientific terms: carbohydrate-induced hypertriglyceridemia. The triglyceride level in the blood always depends on the sugar that is converted into fat in the liver and released into the blood.
So high triglycerides usually mean:
“Your liver is trying to ship out excess energy, and the blood is carrying that overflow around.”
What is HDL?
HDL is often called “good cholesterol,” but that’s too simplistic.
HDL particles are involved in:
- reverse cholesterol transport (bringing cholesterol back from the periphery)
- modulating inflammation and oxidative stress
- acting as part of the immune and repair system in a very dynamic way
When metabolism is working well:
- HDL tends to be more robust (higher and better quality)
- it reflects a system that can clean up and recycle lipids efficiently.
How do you calculate the TG:HDL ratio?
It’s very simple:
TG:HDL ratio = triglycerides ÷ HDL
Using the same units:
- If your labs are in mg/dL (common in the US):
- example: TG 150, HDL 50 → 150 ÷ 50 = 3.0
- If your labs are in mmol/L (common outside US):
- use TG (mmol/L) ÷ HDL (mmol/L) — the ratio concept is the same.
The ratio isn’t magic.
It’s just a quick way to see how much “energy overflow” (TG) you have relative to your cleanup system (HDL).
What numbers are concerning? (With context)
Different studies and clinicians use slightly different thresholds, but a simple functional interpretation often looks like this (for mg/dL units):
- Around 1 or lower → usually very favorable metabolic signal
- Between ~1–2 → often still okay, depending on context and other labs
- Above ~2 → suggests higher probability of insulin resistance / metabolic stress
- Above ~3 and especially >4 → common in more advanced insulin resistance, metabolic syndrome, or carbohydrate-induced hypertriglyceridemia
This is not a diagnosis, and not a replacement for a full clinical picture.
But when someone has:
- fatigue
- belly fat
- creeping glucose
- liver enzyme drift
…and a TG:HDL ratio clearly above 2, the probability of underlying metabolic dysfunction (especially hepatic insulin resistance) is high enough that we should take it seriously and investigate the mechanism.
How high triglycerides tend to push HDL down (the mechanism)
There’s an important pathway here most people never hear about.
When triglycerides are high:
- The blood is full of triglyceride-rich particles (like VLDL).
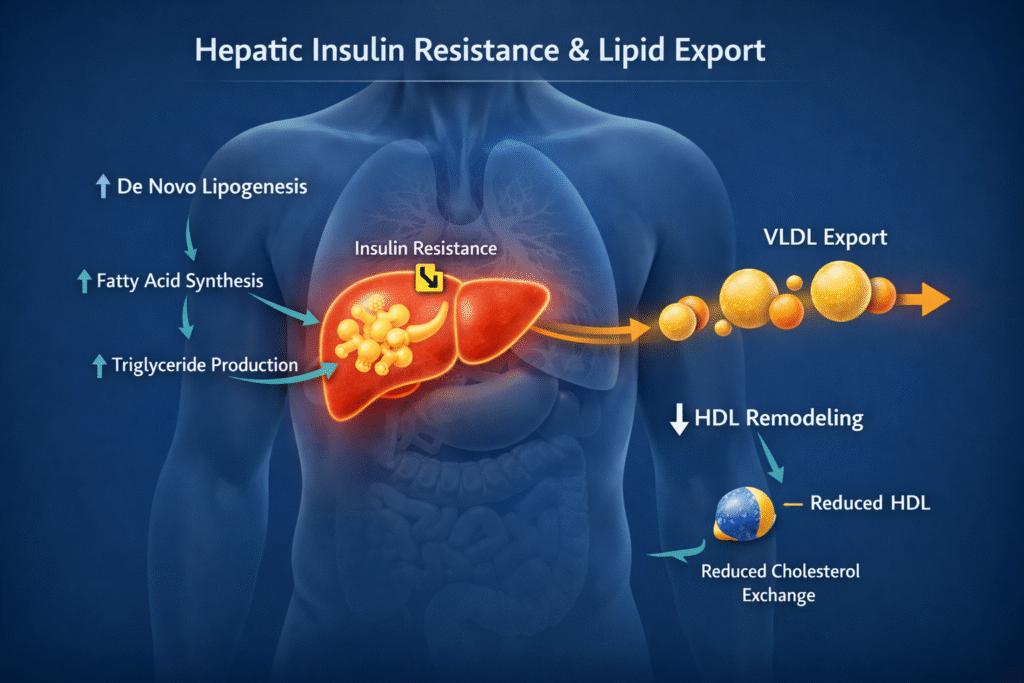
- Through a protein called CETP, triglycerides are exchanged into HDL particles.
- These TG-enriched HDL particles then get acted on by enzymes (like hepatic lipase).
- HDL becomes smaller and more rapidly cleared from the circulation.
End result:
Chronic high triglycerides → HDL gets remodeled, shrinks, and is removed faster → HDL levels often fall or stay unimpressive.
So high TG and low HDL are not independent accidents.
They are two sides of the same disturbed lipid-traffic problem, usually driven by insulin resistance and dietary / lifestyle pressure on the liver.
That’s what the TG:HDL ratio is whispering about — if someone knows how to listen.
If you want a structured interpretation of your labs and symptoms in full physiological context, a metabolic assessment can help clarify what is driving your current state.
What Actually Improves HDL in a Meaningful Way?
It’s tempting to ask:
“What pill raises my HDL?”
“Should I just take niacin?”
Yes, certain drugs and supplements (like niacin) can raise HDL numbers, but large outcome trials haven’t shown clear cardiovascular benefit from simply forcing HDL upward pharmacologically. Raising a number is not the same as restoring the system.
In a systems-biology / functional framework, we focus on the upstream levers that naturally improve HDL quality and, often, its level:
1. Lowering triglyceride pressure
When you reduce the overflow energy forcing the liver to export TG, several things tend to happen:
- TG decreases
- CETP-driven TG loading of HDL lessens
- HDL particles can become larger, more functional, and more stable
Core ways to do this:
- Remove refined carbohydrates and ultra-processed foods
- Reduce constant snacking and late-night eating
- Align meals with circadian rhythm
- Use a protein-forward, nutrient-dense, mostly animal-based pattern to stabilize appetite and energy
2. Improving insulin sensitivity
As insulin sensitivity improves (especially in the liver and muscle):
- liver fat often decreases
- VLDL production falls
- TG levels come down
- HDL tends to recover
Insulin sensitivity is improved by:
- resistance training + walking
- adequate sleep and circadian alignment
- stress modulation
- appropriate caloric load for that person’s context
3. Supporting metabolism with the right fats
Dietary fat is not the enemy. In many people:
- moving away from industrial seed oils
- towards whole-food animal fats and unprocessed fats
- within a metabolically appropriate energy window
helps normalize lipid metabolism.
HDL often responds favorably when:
- carbohydrate load is controlled
- fats are of better quality
- the system is not drowning in energy surplus
4. Where does niacin fit in?
Niacin can raise HDL, and in the past it was used for that purpose. But:
- raising HDL pharmacologically did not consistently translate into better outcomes in large trials
- it can carry side-effects at higher doses
So my focus is not:
“How do we force HDL up?”
But:
“How do we normalize the metabolic traffic so that HDL can reflect a healthier, more functional system?”
If you fix insulin resistance, liver overload, carbohydrate-induced hypertriglyceridemia, and circadian/metabolic stress, HDL usually adapts in the right direction as a downstream effect.
This fits within a broader physiological framework of insulin resistance explained here.
Hepatic Insulin Resistance: The Early Metabolic Breakdown
“The liver is often the first organ where insulin signaling begins to fail, long before glucose spikes or obvious ‘diabetes’ appears.”
Hepatic insulin resistance occurs when the liver no longer responds normally to insulin’s regulatory signals. Instead of properly managing glucose and lipid storage, the resistant liver:
- continues to produce VLDL particles loaded with triglycerides
- increases triglyceride output into the bloodstream
- contributes to rising TG levels relative to HDL
Crucially, this process often happens without dramatic LDL elevation, misleading clinicians who focus solely on LDL-centered risk. (MDPI)
Carbohydrate-Induced Hypertriglyceridemia
Research from the Journal of Lipid Research shows that carbohydrate overload — even in lean individuals — increases triglyceride synthesis and export, especially when the liver’s capacity to safely store or oxidize lipid is exceeded. (JLR) This hypertriglyceridemia is not simply a response to dietary fat — it’s a primary metabolic effect of excess carbohydrate flux combined with hepatic insulin resistance.
See also Insulin Resistance: The Central Mechanism Behind Modern Chronic Disease
Why Conventional LDL-Focused Thinking Falls Short
“Treating lipid numbers without treating their metabolic context is like updating a dashboard without fixing the engine.”
Many clinicians are trained to see cholesterol through an LDL lens. When TG is high, the default tends to be:
- recommend low-fat/high-carb diets
- prescribe statins
- re-test months later
But if the underlying mechanism involves hepatic insulin resistance and carbohydrate-driven VLDL output, neither advice nor statin therapy directly addresses the root driver of that pattern. Large population studies confirm that high TG coupled with low HDL is a hallmark of metabolic syndrome and insulin resistance. Elevated TG:HDL ratios are correlated with atherogenic lipid profiles and metabolic dysfunction more broadly. (ScienceDirect)
Typical Symptom + Lab Pattern That Signals a Deeper Metabolic Story
“When triglycerides rise and HDL does not keep pace, it often reflects deeper hepatic and metabolic dysfunction — not chance.”
Here’s a pattern that often eludes conventional screening:
Symptoms
- Persistent fatigue & afternoon energy crashes
- Brain fog or cognitive softness
- Increasing visceral (belly) fat
- Reduced carb tolerance
- Sleep fragmentation
- Slower recovery
Labs
- Triglycerides rising over time
- HDL appreciably stagnant or dropping
- Fasting glucose creeping upward
- Slightly elevated ALT / liver enzymes
Studies show that individuals with higher TG:HDL ratios have a greater likelihood of insulin resistance, even in normal-weight adults, and that this ratio correlates with surrogate measures like HOMA-IR. (PubMed)
See also Metabolic Flexibility: The Missing Foundation of Modern Metabolic Health
Why Some Standard Dietary Advice Can Backfire
The common “eat less fat, eat more whole grains” advice assumes that all fats inherently raise triglycerides — but in carbohydrate-induced hypertriglyceridemia, the carbohydrate flux itself drives triglyceride production and export. Prioritizing carbohydrates in this metabolic context can worsen lipid export and elevate TG further.
This reflects a mechanistic misunderstanding: it treats numbers as isolated facts, rather than signs of underlying metabolic processes.
A Systems-Biology Approach to Interpretation and Intervention
“Numbers alone don’t heal. What matters is the mechanism they represent.”
A mechanistic approach starts with a map, not a prescription:
Things I evaluate first
- TG:HDL trend over time
- ALT / AST / liver signals
- waist + visceral patterns
- fasting glucose trajectory
- sleep, stress, circadian rhythm
- diet pattern & composition
- training load and recovery
Core levers
- Reduce carbohydrate load strategically
- Focus on nutrient-dense, protein-forward dietary patterns
- Reset meal timing with circadian awareness
- Support gut–liver axis and bile flow
- Resistance training + metabolic capacity building
- Sleep and stress modulation
This isn’t “chasing numbers.” It’s rebalancing physiology so the organs responsible for metabolism can function again — and when that happens, TG:HDL ratios often improve as a downstream effect. (MDPI)
When to Take TG:HDL Seriously
“TG:HDL is not a fringe metric — it’s a robust surrogate for deeper insulin resistance that often precedes overt disease.”
While no single cut-off applies universally, research suggests that higher TG:HDL ratios are predictive of insulin resistance and cardiometabolic risk across diverse populations. (PMC) A steadily rising TG:HDL ratio — even within “normal” ranges — warrants a mechanistic look, especially if accompanied by fatigue, visceral fat gain, or glucose drift.
Metabolic Clarity: How I Work With These Patterns
The clients who benefit most are:
- functionally challenged but not “overtly sick”
- told their labs are fine
- puzzled by persistent symptoms
- trapped in LDL-centric interpretations
In the Metabolic Clarity Session, we:
- integrate labs with symptoms
- map TG:HDL in physiological context
- uncover upstream metabolic drivers
- build a tailored roadmap rooted in systems biology
This is not a generic coaching call. It’s a lab-anchored functional interpretation that informs whether someone proceeds to a structured reset.
See also 90-Day 3R Metabolic Restoration™ — Program Details
If This Sounds Familiar…
“When your body’s story doesn’t match what the lab report says, the TG:HDL ratio can reveal what’s been hidden in plain sight.”
If you recognize this pattern in your own energy, lab trends, or metabolic history — you’re not alone. And you’re not failing. Your system has been trying to tell you something — through TG, HDL, liver signals, and symptoms.
If you want a deeper interpretation with a map that respects biology and context, here’s where you can learn about the Metabolic Clarity Session and how I work with people who have metabolic patterns that the conventional system often overlooks.
See also Metabolic Reset Blueprint for High-Achievers
What does a high TG:HDL ratio usually mean?
A high TG:HDL ratio is frequently associated with hepatic insulin resistance, increased VLDL export, and carbohydrate-induced hypertriglyceridemia. It should be interpreted in metabolic context rather than as an isolated lipid value.
Is TG:HDL more important than LDL?
No single number is “most important,” but TG:HDL often reflects metabolic function, liver stress, and insulin resistance dynamics that LDL alone does not capture. It is a contextual signal — not a replacement marker.
Does a high TG:HDL ratio always indicate disease?
Not necessarily. It is an early-stage physiological signal that may precede overt metabolic disease. It should prompt careful mechanistic interpretation rather than anxiety or reflexive drug escalation.
Can lowering triglycerides improve HDL?
In many cases yes — reducing hepatic TG export, improving insulin sensitivity, and decreasing metabolic overload often leads to improved HDL stability and function as a downstream effect.
Should I take supplements to raise HDL?
Raising HDL pharmacologically or supplementally does not necessarily improve metabolic health. The priority is to address the upstream mechanisms driving triglyceride elevation and hepatic insulin resistance.
Author bio
Morteza Ariana is a Functional Nutrition Practitioner specializing in insulin resistance, type 2 diabetes, and systems-based metabolic restoration. His work focuses on identifying upstream drivers of metabolic dysfunction — including insulin load, liver–gut axis disruption, circadian misalignment, and micronutrient gaps — rather than masking symptoms.
He works with high-performing professionals through a structured 12-week Metabolic Restoration Blueprint designed to restore metabolic flexibility and long-term resilience.
If this resonates, the next step is clarity.
The Metabolic Restoration Blueprint is a structured 12-week framework designed to correct upstream metabolic drivers — not just manage symptoms.
Scientific References
- All referenced studies/topics above point to peer-reviewed science showing:
- TG:HDL ratio correlates with insulin resistance & metabolic syndrome. (ScienceDirect)
- TG:HDL serves as a valid surrogate marker for insulin resistance in diverse populations. (PMC)
- Elevated TG:HDL is linked with adverse lipid phenotypes and cardiometabolic risk. (ScienceDirect)
- Higher TG:HDL ratios correlate with surrogate measures of insulin resistance. (PubMed)
- Abnormal TG/HDL reflects complex lipoprotein dynamics and metabolic stress. (MDPI)